What is a Ventilation/Perfusion Scan?
A Functional Lung Imaging Scan, also known as a Ventilation/Perfusion (V/Q) scan, is a nuclear medicine procedure that uses radioactive material to assess the flow of air and blood in the lungs. It is used by physicians to detect PE, which is a blood clot in the lungs.
V/Q: Reduced Radiation Exposure
Compared with CTPA, the breast radiation dose from V/Q is approximately 40 times less in women and 90 times less in pregnant women.2 That’s why the American Thoracic Society recommends V/Q over CTPA in pregnant patients with a normal chest X-ray.3 The radiation from CTPA is particularly a concern for young women because the breast tissue is particularly radiosensitive due to its higher metabolic activity,4 which is why the Society for Nuclear Medicine and Molecular Imaging recommends avoiding CTPA in young women with a low-pretest probability of PE or a negative D-dimer.5
CTPA delivers a vastly higher radiation dose to the female breast than that delivered by V/Q2

* Estimated CTPA radiation exposure to gravid breast ranges from 1000–2000 mrad, compared to 22–28 mrad from V/Q scan.2
The Society for Academic Emergency Medicine has advocated for evidence-based clinical decision rules to optimize CT utilization, stating that, “Research is needed to refine the indications for CT and to identify the scenarios in which alternatives to traditional CT are most appropriate … and when CT can be avoided without adversely affecting patient-centered care.” 6
ED algorithm with V/Q reduces radiation exposure by 20% 1,2*
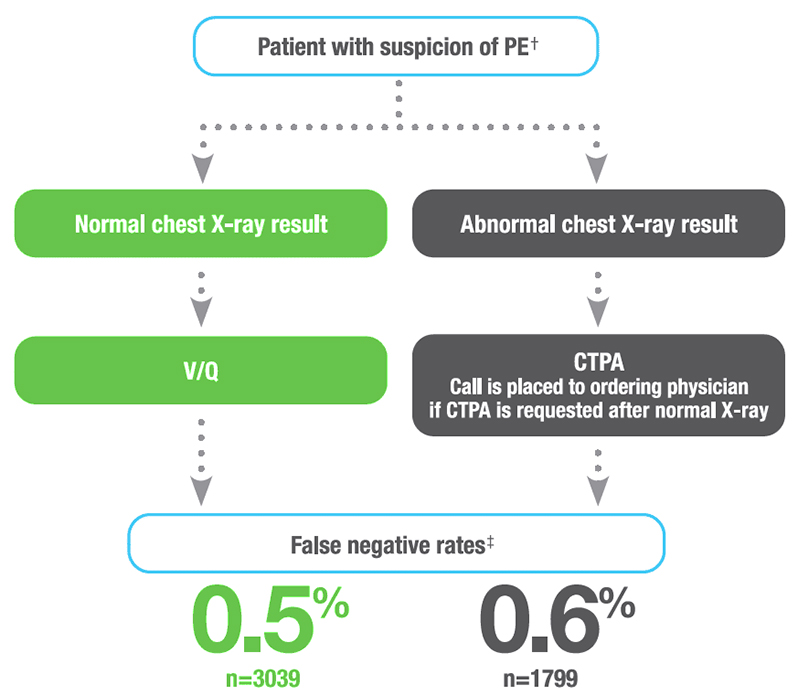
* Validated at one of the busiest emergency departments in the U.S.
† Unstable patients undergo CTPA.
‡ For PE alone.
An algorithm that incorporates V/Q scans to evaluate patients for PE in the emergency department has been shown to reduce overall patient radiation exposure by 20%.1 This approach uses chest radiography as an initial step to triage all suspected PE cases. Patients with a normal X-ray result underwent a V/Q scan, and patients with abnormal results received a CTPA. In the same study involving more than 2,000 patients at one hospital that employed this algorithm showed that the false-negative rates were 0.5% and 0.6% for V/Q and CTPA respectively, demonstrating that there was no statistical difference inoutcomes for both procedures.1,2 The use of other preliminary diagnostic criteria/ triage variables, such as validated prediction rules for risk stratification and screening with D-dimer assay, can be effectively utilized as well to diagnose PE while minimizing risk of unnecessary radiation burden.7
V/Q: The Right Treatment for the Right Patient at the Right Time
Although CTPA has been demonstrated to be more sensitive than V/Q, with a false-negative rate of 0.4% vs 1%, respectively, during 3 months of follow-up, its use inadvertently resulted in a significantly greater number of venous thromboembolism diagnoses than did V/Q (19.2% vs 14.2%; P=0.01).8 There is evidence that these minor, subsegmental PEs may not be clinically relevant as a diagnosis or for therapy. Three epidemiological studies found that despite detecting twice as many PEs as V/Q, CTPA did not reduce patient mortality.9-11 By detecting clinically insignificant PEs, CTPA may cause patients to undergo unnecessary tests and treatments—such as anticoagulation therapy—increasing the risk for complications and the total cost of care. Available data, in fact, indicate that patients diagnosed with subsegmental PEs via CTPA are more likely to experience complications from anticoagulation than adverse outcomes from recurrent thromboembolism.12,13
Recognizing the risk associated with overdiagnosis and overtreatment, the American College of Chest Physicians recommends clinical surveillance over anticoagulation in patients with a subsegmental PE (no involvement of more proximal pulmonary arteries) and no proximal deep vein thrombosis in the legs who have a low risk for recurrent venous thrombolism.14
Several decades ago, ventilation-perfusion (V/Q) scan interpretation of pulmonary embolism was performed using probability-based assessments: normal, very low probability and low-probability. Although this approach served well the technology at the time,it was not well-understood by many clinicians. With the development of more advanced imaging equipment and new technology, the Nuclear medicine community is evolving in the diagnostic approach of PE.
Recent advancements allow physicians to obtain the same degree of interpretive clarity with a V/Q scan as they can with CTPA. Some hospitals have implemented a simplified interpretative scheme for V/Q that mimics that used with CTPA—PE-absent, PE-present, and nondiagnostic. Adoption of this trinary V/Q reporting system has been shown to produce a comparable false-negative rate compared with the traditional, probability-based interpretive scheme.15 More importantly, the trinary V/Q reporting system also facilitated communication of V/Q results with referring physicians, and radiology and nuclear medicine residents have expressed much greater comfort interpreting V/Q studies.15 With minimal training, an experienced radiologist using this interpretation scheme can read a V/Q study in just a few minutes.
Trinary scheme simplifies V/Q interpretation and reporting15
Findings consistent with PE: If this finding is discordant with objective clinical assessment, further investigation is warranted.
No evidence of PE: If this finding is discordant with objective clinical assessment, further investigation is warranted.
Nondiagnostic study: Further study with V/Q (CTPA) may be helpful.
Reference:
1. Stein EG, Haramati LB, Chamarthy M et al. Success of a safe and simple algorithm to reduced use of CT pulmonary angiography in the emergency department. Am J Roentgenol. 2010;194:392–397.
2. Da Silva R, Shah M, Freeman LM. Ventilation-perfusion (V/Q) lung scintigraphy: a long journey to a renewed position of prominence in diagnosing pulmonary embolism. Clin Transl Imaging. 2014;2:369–378.
3. Leung AN, Bull TN, Jaeschke R, et al. An Official American Thoracic Society/Society of Thoracic Radiology Clinical Practice Guideline: Evaluation of Suspected Pulmonary Embolism In Pregnancy. Am J Respir Crit Care Med. 2011;184(5): 1200–1208.
4. Schembri GP, Miller AE, Smart R. Radiation dosimetry and safety issues in the investigation of pulmonary embolism. Semin Nucl Med. 2010;40(6):442-454.
5. Society for Nuclear Medicine and Molecular Imaging. Choosing Wisely. Available at: http://www.snmmi.org/ClinicalPractice/content.aspx?ItemNumber=9914. Accessed on June 24, 2016.
6. Moore CL, Broder J, Gunn ML, et al. Comparative Effectiveness Research: Alternatives to “Traditional” Computed Tomography Use in the Acute Care Setting. Acad Emerg Med. 2015;22(12):1465–1473.
7. Wilbur J and Shian B. Diagnosis of deep vein thrombosis and pulmonary embolism. Am Fam Physician. 2012;86(10):913-919.
8. Anderson DR, Kahn SR, Rodger MA, et al. Computed tomographic pulmonary angiography vs. ventilation/perfusion lung scanning in patients with suspected pulmonary embolism. JAMA. 2007;298:2743–2753.
9. Burge AJ, Freeman KD, Klapper PI, Haramati LB. Increased diagnosis of pulmonary embolism without a corresponding decline in mortality during the CT era. Clin Radiol. 2008;63:381–386.
10. Sheh SH, Bellin E, Freeman KD, Haramati LB. Pulmonary embolism diagnosis and mortality with CT pulmonary angiography versus ventilation perfusion scintigraphy: evidence of over diagnosis with CT? Am J Roentgenol. 2012;198:1340–1345.
11. Wiener RS, Schwartz LM, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171:831–837.
12. Carrier M, Righini M, Wells PS, et al. Subsegmental pulmonary embolism diagnosed by computed tomography: incidence and clinical implications. A systematic review and meta-analysis of the management outcome studies. J Thromb Haemost. 2010;8(8):1716–1722.
13. Donato AA, Khoche S, Santora J, Wagner B. Clinical outcomes in patients with isolated subsegmental pulmonary emboli diagnosed by multidetector CT pulmonary angiography. Thromb Res. 2010;126(4):e266-70.
14. Kearon C, Akl EA, Joseph Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016;149(2):315–352.
15. Glaser JE, Chamarthy M, Haramati L, et al. Successful and safe implementation of a trinary interpretation and reporting strategy for V/Q lung scintigraphy. J Nucl Med. 2011;52:1–5.
DISCLAIMER:
This information is not intended as medical advice. Responsibility for patient care resides with the healthcare professional on the basis of his or her professional license, experience and knowledge of the patient. For full Prescribing Information including indications, contraindications, warnings, precautions and adverse events, please see the appropriate product labeling.